















 Cooled Radiofrequency Ablation (RFA)
Cooled Radiofrequency Ablation (RFA) Tined Radiofrequency Ablation (RFA)
Tined Radiofrequency Ablation (RFA) Conventional Radiofrequency Ablation (RFA)
Conventional Radiofrequency Ablation (RFA) RFA Equipment & Accessories
RFA Equipment & Accessories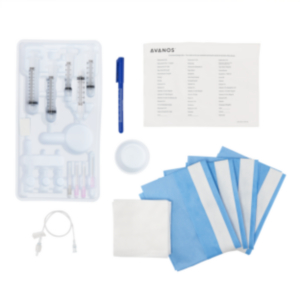 Needles, Kits, and Trays
Needles, Kits, and Trays Elastomeric Pain Pumps and Kits
Elastomeric Pain Pumps and Kits Needles, Kits, and Trays (Incisional and PNB)
Needles, Kits, and Trays (Incisional and PNB) Cryo Compression Control Unit Systems
Cryo Compression Control Unit Systems Cryo Compression Sleeves and Wraps
Cryo Compression Sleeves and Wraps Feeding Tube Placement Device
Feeding Tube Placement Device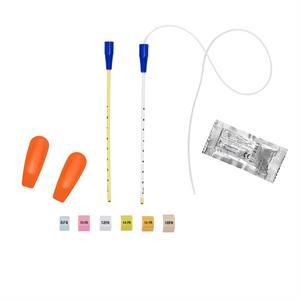 Feeding Tube Retention Systems
Feeding Tube Retention Systems Declogging and Decompression
Declogging and Decompression Introducer Kits and Accessories
Introducer Kits and Accessories Feeding Tube Extension Sets and Adapters
Feeding Tube Extension Sets and Adapters Enteral Medication Preparation & Delivery
Enteral Medication Preparation & Delivery Feeding Accessories
Feeding Accessories Feeding Pumps
Feeding Pumps Feeding Syringes
Feeding Syringes Feeding Tubes and Extension Sets
Feeding Tubes and Extension Sets Lumbar Puncture Trays and Needles
Lumbar Puncture Trays and Needles Oral Care/Colostrum Kits and Components
Oral Care/Colostrum Kits and Components Urinary Catheters & Kits
Urinary Catheters & Kits
Redefine the Initial Placement Experience
Initial Placement is Associated with Low Complications1–3
Avanos Initial Placement Kit, including the proprietary T-Fasteners and telescopic dilator, is designed to aid in an efficient initial placement of a balloon-retained feeding tube.† Clinical literature reports that placement of MIC* & MIC-KEY* feeding tubes using the Avanos Initial Placement Kit is safe, effective and minimally invasive.†
PROPRIETARY INITIAL PLACEMENT KIT TECHNOLOGY
Telescoping Sequential Dilators
Using telescopic dilators from the Avanos Initial Placement Kit resulted in less sedation, allowing for faster recovery and discharge time compared to procedures with sequential dilators. † 4
You can reach desired dilation with a single, proprietary telescoping device.†


SAF-T-PEXY* T-Fasteners
The Gastrointestinal Anchor Set with SAF-T-PEXY* T-Fasteners is intended to affix the stomach to the anterior abdominal wall facilitating primary placement of the MIC* and MIC-KEY* brand Enteral Feeding Tubes. It is recommended that these T-Fasteners be used only with the MIC* and MIC-KEY* brand Enteral Feeding Tubes.
The SAF-T-PEXY* device contains 3/0 Biosyn® synthetic absorbable suture that in non-clinical studies retained tensile strength to approximately 75% of U.S.P. and E.P. minimum knot strength at 14 days and approximately 40% at 21 days post-implantation. Absorption of the suture is essentially complete within 90 to 110 days.
Benefits of Initially Placing a Balloon-Retained Tube
Gastrostomy buttons can be placed initially without the need for a mature stoma, which may be an appealing option for active adult patients.5 Numerous studies also show initial placement is safe, effective, and technically feasible for infants and pediatric patients.6–11
Placing a balloon-retained gastrostomy tube initially with an Initial Placement Kit…
- Significantly avoids the need for a second procedure for tube replacement under general anesthesia† 2
- Minimizes the risk of procedure-related morbidity and leads to overall improvement in the quality of life8
- Lowers the rate of infection and sedation requirements, which allows for faster recovery and shortened hospital length of stay4,12
- Provides good anatomical delineation, a single incision, and elimination of radiation and its associated risks11
- Optimally attaches the stomach to the abdominal wall13–15
.
Proven Across Specialties
Endoscopic Techniques
- Initial placement with an endoscopic technique allows for direct visualization, which can help avoid bleeding, penetration of the bowel, and partial obstruction due to tube location when compared with blind placement.16
- Martins et al shows infection scores were marginally higher with the pull-PEG procedure than with initial placement.17
- The percent of tube dislodgement associated with major complications was higher with pull-PEG procedures, although this difference was not statistically significant.18
Fluoroscopic Techniques
- Initial placement with fluoroscopic guidance is safe, technically feasible, and effective compared with pull-PEG procedures for both pediatric and adult patients.1,6,19–21
- Sheehan et al found benefits of this procedure include a single visit to the IR suite (versus a second visit for ‘button’ insertion), reduced risk of inadvertent tube removal, and improved cosmetic results.22
- Studies have shown initial placement with fluoroscopic guidance can shorten hospital length of stay and can even be performed as an outpatient procedure for some patients.4,23,24
- Dolan et al found that pairing this procedure with an expedited feeding protocol is a safe and cost-comparable alternative to overnight hospitalization, the current standard of care.24
- Maroun et al found initial placement required less sedation, allowing for faster recovery and shortened hospital length of stay.4
Laparoscopic Techniques
- Livingston et al found initial placement laparoscopic guidance removes the need for post-procedure tube exchanges.23
- Studies have shown initial placement with laparoscopic guidance is safe and effective for both pediatric and adult patients.3,7,13,14,25
- Initial placement with laparoscopic guidance is a minimally invasive procedure associated with lower post-operative complications.7,26
- This procedure is associated with a decrease in short-term surgical site infections.26
- Due to its lower complication rate, initial placement with laparoscopic guidance may be a preferred technique for patients who are not eligible for surgical procedures.25
Initial Placement Kit Components
Avanos offers initial placement kits for G Tubes and J / GJ Tubes which can be used in endoscopic, radiologic, and laparoscopic placements.
| Differences in Kits | Endoscopic/Radiologic | Laparoscopic |
| Gastrostomy Tubes | Serial Dilator SAF-T-PEXY T-Fasteners (4) Safety Introducer Needle, 18ga Safety Scalpel with #11 Blade Forceps 12mL Luer Slip Syringe OTW Stoma Measuring Device 0.035in x 80cm Guidewire | Serial Dilator SAF-T-PEXY T-Fasteners (4) Safety Introducer Needle, 18ga Safety Scalpel with #11 Blade Forceps 12mL Luer Slip Syringe OTW Stoma Measuring Device 0.035in x 80cm Guidewire Sterilization Wrap |
| Gastro-Jejunal and Jejunal Tubes | Serial Dilator SAF-T-PEXY T-Fasteners (4) Safety Introducer Needle, 18ga Safety Scalpel with #11 Blade Forceps 12mL Luer Slip Syringe OTW Stoma Measuring Device 5Fr x 75cm Seeking Catheter | Serial Dilator SAF-T-PEXY T-Fasteners (4) Safety Introducer Needle, 18ga Safety Scalpel with #11 Blade Forceps 12mL Luer Slip Syringe OTW Stoma Measuring Device 5Fr x 75cm Seeking Catheter Sterilization Wrap |
NOTE: Your facility should source the following additional components in order to complete the procedure.
- Chloraprep
- Extra Scalpel
- Extra Set of SAF-T-PEXY
- Fenestrated Drape
- Lidocaine
- Lidocaine needle
- Lubricant
- MIC* or MIC-KEY* Feeding Tube
- Povidone Iodine
- Scissors
- Shaver
- Split gauze
- Sterile Gloves
- Sterile water
Compatible Products






FAQ for AVANOS* IPK
1. What feeding tube french size corresponds to each initial placement kit?
The feeding tube should be 4 french sizes smaller than the initial placement kit. For example, if you are placing a 14Fr feeding tube, then you should use an 18Fr initial placement kit. Please reference the IFU for more details.
2. Do initial placement kits come with a feeding tube?
Feeding tubes are sold separately from initial placement kits.
3. What type of guidewire is included in the initial placement kit?
Guidewire Details (SPEC-09456)
- Length: 31.5 in
- Diameter: 0.035 in
- Material: PTFE coated stainless steel
4. How soon after placement can enteral feeding begin?
Begin feeding only after confirmation of proper patency and placement, according to physician instructions.
5. Can low-profile and standard length tubes be placed initially?
The AVANOS* Introducer Kit is intended to facilitate primary placement of the MIC* Feeding Tube and MIC-KEY* Low-Profile Feeding Tube.
6. Do I need to cut the sutures of the SAF-T-PEXY and what is the recommended time for sutures to be in place before cutting them?
The sutures may be left to be absorbed or they may be cut when deemed appropriate by the placing physician. Letting the sutures be absorbed or cutting them will allow the T-bars to pass through the gastrointestinal system. After the sutures dissolve (or are cut) the suture locks may be removed and discarded.
Note: It is recommended not to cut the sutures within two weeks post-procedure.
7. What is the post-procedure care after initial placement?
- Inspect the stoma and gastropexy sites daily and assess for signs of infection, including: redness, irritation, edema, swelling, tenderness, warmth, rashes, purulent or gastrointestinal drainage. Assess for any signs of pain, pressure or discomfort.
- After the assessment, routine care should include cleansing the skin around the stoma site and gastropexy sites with warm water and mild soap, using a circular motion, moving from the tube and external bolsters outward, followed by a thorough rinsing and drying well.
Join healthcare professionals worldwide who rely on the Avanos Initial Placement Kit as part of their efforts to support safe placement and patient care.
Disclaimer: The information provided is for educational purposes only and is not intended to replace discussions with a healthcare provider. There are inherent risks in all medical devices. Please refer to the product labeling for indications, cautions, warnings and contraindications.
1. Power S, Kavanagh LN, Shields MC, et al. Insertion of Balloon Retained Gastrostomy Buttons: A 5-Year Retrospective Review of 260 Patients. Cardiovasc Intervent Radiol. 2013;36(2):484-491. doi:10.1007/s00270-012-0456-3
2. Jean-Bart C C, Aumar M, Ley D, et al. Complications of one-step button percutaneous endoscopic gastrostomy in children. Eur J Pediatr. 2023;182(4):1665-1672. doi:10.1007/s00431-023-04822-7
3. Serrano Aguayo P, Gros Herguido N, Parejo Campos J, et al. New laparoscopic assisted percutaneous gastrostomy. Description and comparison with others gastrostomy types. Clin Nutr ESPEN. 2016;16:24-29. doi:10.1016/j.clnesp.2016.08.004
4. Maroun G, Pugash R, Meirovich H, David E. Efficiency and Safety of Balloon-Assisted Gastrostomy. Cardiovasc Intervent Radiol. 2021;44(9):1423-1429. doi:10.1007/s00270-021-02865-7
5. Lyon SM, Haslam PJ, Duke DM, McGrath FP, Lee MJ. De Novo Placement of Button Gastrostomy Catheters in an Adult Population: Experience in 53 Patients. J Vasc Interv Radiol. 2003;14(10):1283-1289. doi:10.1097/01.RVI.0000092901.73329.EB
6. Gill AE, Gallagher N, McElhanon BO, Painter AR, Gold BD, Hawkins CM. Image-guided placement of percutaneous de novo low-profile gastrojejunostomy tubes in the pediatric population: a study of feasibility and efficacy. Pediatr Radiol. 2018;48(6):882-888. doi:10.1007/s00247-018-4082-3
7. Kozlov Y, Novozhilov V, Kovalkov KA. Comparison of Two Laparoscopic Techniques for Gastropexy in Children. J Laparoendosc Adv Surg Tech. 2015;25(12):1057-1062. doi:10.1089/lap.2015.0091
8. Stehr W, Farrell MK, Lucky AW, Johnson ND, Racadio JM, Azizkhan RG. Non-endoscopic percutaneous gastrostomy placement in children with recessive dystrophic epidermolysis bullosa. Pediatr Surg Int. 2008;24(3):349-354. doi:10.1007/s00383-007-2100-x
9. Michaud L, Robert‐Dehault A, Coopman S, Guimber D, Turck D, Gottrand F. One‐step Percutaneous Gastrojejunostomy in Early Infancy. J Pediatr Gastroenterol Nutr. 2012;54(6):820-821. doi:10.1097/MPG.0b013e31824d970f
10. Jacob A, Delesalle D, Coopman S, et al. Safety of the One-Step Percutaneous Endoscopic Gastrostomy Button in Children. J Pediatr. 2015;166(6):1526-1528. doi:10.1016/j.jpeds.2015.03.008
11. Church JT, Speck KE, Jarboe MD. Ultrasound-guided gastrostomy tube placement: A case series. J Pediatr Surg. 2017;52(7):1210-1214. doi:10.1016/j.jpedsurg.2017.03.061
12. Alhussaini B, Al-Dajani N. Infection rate inpercutaneous endoscopic gastrostomy versus one-step gastrostomy in hospitalized children at a tertiary care hospital in jeddah, saudi arabia. Int J Curr Res. 2020;12(8):13034-13037.
13. Hassan SF, Pimpalwar AP. Modified laparoendoscopic gastrostomy tube (LEGT) placement. Pediatr Surg Int. 2011;27(11):1249-1254. doi:10.1007/s00383-011-2977-2
14. Scalise PN, Durgin JM, Koo DC, et al. Outcomes of laparoscopic gastrostomy in children with and without the use of a modified T-fastener technique. Surgery. 2023;174(3):698-702. doi:10.1016/j.surg.2023.05.013
15. Durgin JM, Slatnick B, Yang A, et al. The Paired T-Fastener Technique: A Bolster-Free Gastropexy for Laparoscopic Gastrostomy Tube Placement. J Laparoendosc Adv Surg Tech. 2021;31(12):1431-1435. doi:10.1089/lap.2021.0336
16. Yuwono M, Holland R, Acierno S, Pickens M, Lustig D. Is Primary Endoscopic Guided Placement of Low Profile Gastrostomy Tube (Mic-Key®) Feasible in Pediatric Patients? Am J Gastroenterol. 2010;105:S387.
17. Martins FP, Sousa MCBD, Ferrari AP. New “introducer” PEG-gastropexy with T fasteners: a pilot study. Arq Gastroenterol. 2011;48(4):231-235. doi:10.1590/S0004-28032011000400003
18. Kulvatunyou N, Zimmerman SA, Sadoun M, et al. Comparing Outcomes Between “Pull” Versus “Push” Percutaneous Endoscopic Gastrostomy in Acute Care Surgery: Under-Reported Pull Percutaneous Endoscopic Gastrostomy Incidence of Tube Dislodgement. J Surg Res. 2018;232:56-62. doi:10.1016/j.jss.2018.06.011
19. Maxwell CI, Hilden K, Glasgow RE, Ollerenshaw J, Carlisle JG, Fang JC. Evaluation of Gastropexy and Stoma Tract Maturation Using a Novel Introducer Kit for Percutaneous Gastrostomy in a Porcine Model. J Parenter Enter Nutr. 2011;35(5):630-635. doi:10.1177/0148607111413596
20. Gallo CJR, Agassi AM, Johnson DY, et al. Percutaneous Gastrojejunostomy Tube Insertion in Patients with Surgical Gastrojejunal Anastomoses: Analysis of Success Rates and Durability. J Vasc Interv Radiol. 2021;32(2):277-281. doi:10.1016/j.jvir.2020.10.001
21. Hawkins CM, Somasundaram A, Shah J, Variyam D, Gill AE. Mid-to-long-term outcomes with image-guided placement of de novo low-profile gastrojejunostomy tubes in pediatric patients. Clin Imaging. 2023;103:109991. doi:10.1016/j.clinimag.2023.109991
22. Sheehan M, O’Brien C, Killick D, et al. An 8‐year, single‐centre experience of primary image‐guided insertion of ‘button’ gastrostomy catheters: Technical and clinical results. J Med Imaging Radiat Oncol. 2023;67(5):519-525. doi:10.1111/1754-9485.13501
23. Livingston MH, Pepe D, Jones S, Bütter A, Merritt NH. Laparoscopic-assisted percutaneous endoscopic gastrostomy: insertion of a skin-level device using a tear-away sheath. Can J Surg. 2015;58(4):264-268. doi:10.1503/cjs.014814
24. Dolan RS, Duszak R, Bercu ZL, Martin JG, Newsome J, Kokabi N. Comparing the Safety and Cost of Image-Guided Percutaneous Gastrostomy Tube Placement in the Outpatient Versus Overnight Observation Setting in a Single-Center Retrospective Study. Acad Radiol. 2021;28(8):1081-1085. doi:10.1016/j.acra.2020.04.044
25. Lapkus M, DeMare AM, England AL, Akay B, Brahmamdam P. Pediatric Laparoscopic Gastrostomy With T-Fasteners: A Technique to Decrease Surgical Site Infection. Am Surg. 2023;89(6):2989-2992. doi:10.1177/00031348221101589
26. Cave JJ, Chacon CS, Ross AR, et al. Percutaneous endoscopic primary gastrostomy button (PEG-B) is safe and significantly reduces the need for general anaesthetic tube changes in children when compared to the percutaneous endoscopic gastrostomy tube (PEG-T): a prospective study. J Pediatr Endosc Surg. 2019;1(4):143-148. doi:10.1007/s42804-020-00042-0